Frequently Asked Questions
Q: It seems like there are a lot of different names out there for Munchausen by Proxy, such as Factitious Disorder Imposed on Another and Medical Child Abuse. Which is the appropriate term?
As you’ve inferred, there are quite a few terms that have been applied to this form of maltreatment. Professor Roy Meadow coined the term “Munchausen Syndrome by Proxy” in 1977, and that term may be the best known of all. Lately, I prefer the term “medical child abuse (MCA),” because it is descriptive and easier to understand. But, in 2013, the American Psychiatric Association decided that this abusive behavior was associated with a mental disorder they call “Factitious Disorder Imposed on Another” (FDIA). So, I sometimes use MCA and sometimes FDIA, depending on the issues in a particular case. But every individual who engages in MCA, whether they meet criteria for FDIA as well, is a perpetrator, and that point can never be forgotten. Unfortunately, the evolving terminology has been used by some attorneys and others to try to debunk the entire phenomenon as “psychobabble,” but that is simply a bald attempt to delegitimize it and exonerate the perpetrator.
Q: How common do you believe MBP really is?
I strongly believe that most cases are never recognized. Instead, the child undergoes years of suffering without any doctor, relative, or friend ever realizing that the mother herself is the reason the child is so sick. It is not nearly as rare as many people think. It is estimated that there are 600 to 1,200 new cases each year in the United States (based on research done in the United Kingdom). This makes it uncommon compared to other forms of maltreatment such as sexual abuse, but doctors and others shouldn’t be blind to the possibility when risk factors or odd maternal behaviors are present. I say “maternal behaviors” because 96 percent of perpetrators are the child’s mother. This may be because it is largely a crime of opportunity, and mothers in most societies have much more and consistent access to the children and pediatricians than fathers or other partners.
Q: What are the differences between Munchausen Syndrome, Munchausen by Proxy, and Munchausen by Internet?
If I hadn’t been immersed in this work for so long, I too might be confused. There is no mnemonic that I know of, but all you really need to know is that “Munchausen Syndrome” is the most severe and chronic form of factitious disorder (when one fabricates illness in oneself). The American Psychiatric Association is no longer using the term “Munchausen” for any ailment, but the public (and most professionals) haven’t given it up! Munchausen by Proxy is a form of medical abuse that victimizes others (usually children, the elderly, or pets). Munchausen by Internet is when the same behaviors occur either partly or entirely online.
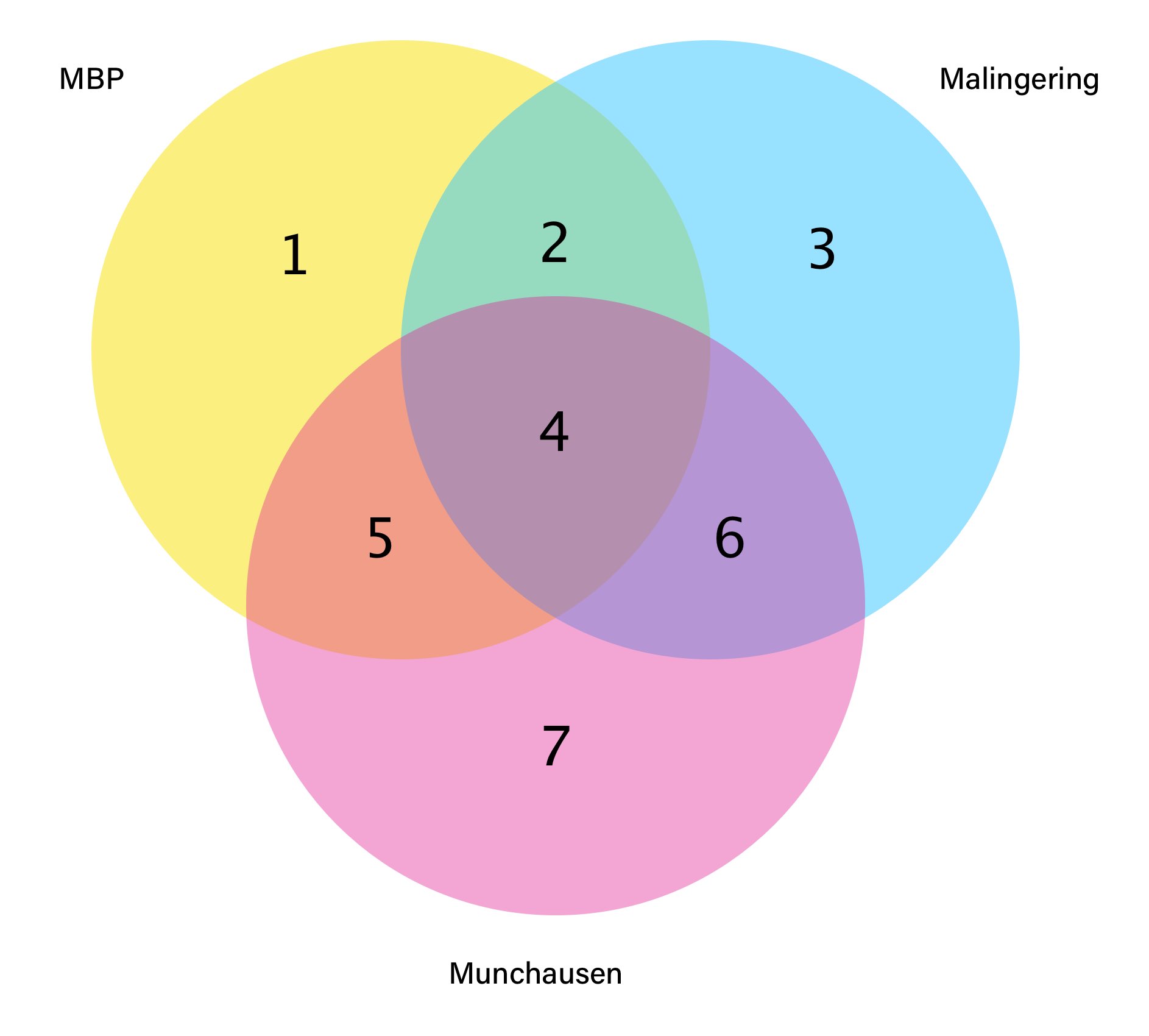
Section 1
Medical deception with underlying psychiatric disorder of Factitious Disorder Imposed on Another (FDIA)
Section 2
Perpetuates Medical Child Abuse through illness or injury in a child under their care to get both emotional gratification and external gain
Section 3
Sole motive is external and usually material, not internal and psychological.
Section 4
Receives resources such as money and attention for enacted or induced illness in self and another
Section 5
Motive is psychological for medical deception involving oneself and another
Section 6
Underlying psychiatric disorder of Factitious Disorder Imposed on Self (FDIS) as well as pursuit of external gain
Section 7
Invents, exaggerates, or induces illness or injury on self for emotional gain
Q: Is there a spectrum of how serious Munchausen by Proxy cases are?
MBP always involves emotional abuse and generally involves physical abuse as well (at the hands of the perpetrator and often, unwittingly, doctors and/or others). But there are gradations to this form of maltreatment as with other forms of abuse and neglect. For instance, six to nine percent of known MBP cases culminate in the death of the victim (at least among published reports), and one would obviously view those cases as irreparably severe, unlike those that have no lasting physical effects.
Q: What are the warning signs of Munchausen by Proxy?
According to the American Professional Society on the Abuse of Children here are some common signs of abuse to watch out for:
- Reported symptoms or behaviors that are not congruent with observations. For example, the abuser says the child cannot eat, and yet the child is observed eating without the adverse symptoms reported by the abuser.
- Discrepancy between the abuser’s reports of the child’s medical history and the medical record.
- Extensive medical assessments do not identify a medical explanation for the child’s reported problems.
- Unexplained worsening of symptoms or new symptoms that correlate with abuser’s visitation or shortly thereafter.
- Laboratory findings that do not make medical sense, are clinically impossible or implausible, or identify chemicals, medications, or contaminants that should not be present.
- Symptoms resolve or improve when the child is separated and well protected from the influence and control of the abuser.
- Other individuals in the home or the caregiver have or have had unusual or unexplained illnesses or conditions.
- Animals in the home have unusual or unexplained illnesses or conditions – possibly similar to the child’s presentation (e.g., seizure disorder).
- Conditions or illnesses significantly improve or disappear in one child and then appear in another child, such as when another child is born and the new child begins to have similar or other unexplained symptoms.
- Caregiver is reluctant to provide medical records, claims that past records are not available, or refuses to allow medical providers to discuss care with previous medical providers.
- The abuser reports that the other parent is not involved, does not want to be involved, and is not reachable.
- A parent, child, or other family member expresses concern about possible falsification or high-healthcare utilization.
Observations of clear falsification or induction by the caregiver. This may take the form of false recounting of past medical recommendations, test or exam results, conditions, or diagnoses.
Q: What is the difference between Munchausen by Proxy and Malingering by Proxy?
Munchausen by Proxy and Malingering by Proxy have a lot in common—indeed, the essential features are the same. Both involve the fabrication or induction of signs and symptoms (physical and/or psychological) in another person (or even a pet). But in Munchausen by Proxy (MBP), the principal goal is intangible; that is, the perpetrator is after some form of emotional satisfaction, perhaps by obtaining attention and nurturance as the parent of a child whose illness is defying diagnosis and treatment. In contrast, malingering by proxy (MAL-BP) is primarily in pursuit of an external—and usually tangible—incentive. These external goals can include disability payments; gifts and donations; evasion of criminal prosecution or military service; etc. Note the important point that MBP and MAL-BP can co-exist because people often have more than one reason for engaging in a behavior. A particular case can also shift from MBP to MAL-BP or vice versa.
Q: How does Munchausen by Proxy affect survivors of this abuse once they’ve left home?
The limited research that exists on adult survivors shows that victims tend to have PTSD and often fear even medically necessary treatment. They may avoid psychological treatment for the same reason, especially if the mother’s deceptions involved false psychological claims, such as false ADHD, bipolar disorder, autism, developmental disabilities, and the like. A few even develop factitious disorder themselves, as if to “master” the trauma by making it their own. Many survivors were pre-verbal or early-verbal when the MBP took place, so needless to say, their memories of the incidents are limited or absent. Others have trouble with “reality testing,” or discerning generally what is true and real and what is not wholly true. So, it isn’t at all surprising that many victims are deeply affected and have emotional issues to combat. There certainly needs to be more research done to determine how to best help adult survivors recover and heal.
Courageous survivors have come forward to share their experiences including, notably, Mary Bryk and Hannah Milbrandt, whose stories I’ve linked to below. I also spoke to a number of survivors for my most recent book, Dying to Be Ill. They recount their splendid victories over the past in personal narratives that discuss their paths to healing.
Q: It seems like most MBP perpetrators are female; why is that?
Almost all the known perpetrators are not only female, but the mother of the victim(s). There are more than 700 studies from around the world that affirm this finding. I believe that MBP is in some ways a behavior based in opportunity, and, as the primary caregivers in most situations, mothers have access and credibility when it comes to the alleged health or illness of their children. MBP families tend also to have a tacit or explicit assignment of “traditional” roles where the father is the breadwinner and the mother tends to all matters involving the home and children. Alternatively, the father is either absent or largely unavailable in many of these situations. Female perpetrators tend to have more subtle methods of abuse than males, who are often more outwardly violent.
Q: What should I do if I suspect someone in my family is an MBP perpetrator?
First, you need to understand as much as you can about MBP as these cases are complex, and it is often tricky for loved ones to intervene. I recommend reading everything I’ve listed about MBP (link to MBP section), including this piece from Detective Mike Weber. You can also refer to my books on the subject because they will educate you. Once you have a good understanding, you will be equipped to decide whether to proceed with a sound, organized report to your county child protection agency or even the police. You can also reach out to the folks at Childhelp, a fine organization which runs a national abuse hotline.
Prematurely alerting the alleged perpetrator to the suspicions can lead them to flee with the child; seriously sicken the child to “prove” their case; sign the child out of the hospital against medical advice; and the like. I would recommend that a skilled therapist who has at least some knowledge about MBP, and who is willing to learn more about it, assist in each case because the facts and situation may require a different approach. You also would need to cooperate with the authorities and remain available to assist, if possible. Of course, mandated reporters such as physicians and other healthcare professionals must make the MBP report at the time they become reasonably suspicious that it is occurring, even in the absence of confirmation. Certainly, as I suggested, you need to be aware of the warning signs of MBP, as listed above.
Because record-keeping can be crucial for cases that go to court, it’s imperative that you keep a record of your communications with the suspected perpetrator, including details of various incidents, photos, text messages, emails, and screenshots of social media posts.
Q: Are MBP perpetrators treatable?
The typical reaction upon confrontation of the mother is firm denial, even when there are video recordings of her abusing the child. As researchers from UCLA and Stanford have recently pointed out, therapy for perpetrators can rarely proceed if they are denying the reality of their own behavior. They are unable to engage with the therapist. There are, of course, some exceptions. In my latest book, Dying to be Ill: True Stories of Medical Deception, I have a chapter entitled, “Healing,” in which I recount the case of a mother who had lied about her baby having constant seizures despite medication, claiming further that previous children she had had died of seizures. Despite her initially denying she had ever lied, she improved over the next few years with psychotherapy, treatment for depression, parenting classes, and further education. She improved remarkably, and eventually reunification with the child could occur. It has been very successful. But such cases are very uncommon, even among cases that are relatively minor in severity.
Q: What does a perpetrator ‘get’ out of committing MBP?
The principal goal is internal, though there may be concurrent external goals too (such as obtaining money from GoFundMe accounts). One does not rule out the other. The internal goal is a form of emotional gratification, in most cases from attention and sympathy from appearing to be the indefatigable caregiver of a child with a baffling and/or serious illness. The care and concern that result can be seductive and help to continue or increase the maltreatment. Other perpetrators feel a loss of control in their own lives and being able to mislead (and associate with) doctors and other high-status people allows them once again to feel “in control.” Some have a sadistic streak that fuels the abusive behaviors, and others are rageful that the child has usurped their freedom. Still others lack a clear sense of self (they lack “ego strength” and a sense of self-definition) and being the mother of a terribly ill child becomes their identity, which paradoxically reduces their general anxiety about life.
Perpetrators and those who study them often liken the behavior to an addiction or compulsion: these abusers experience an impulse to harm that can feel irresistible, and some experience a build-up of tension and anxiety that seems to be reduced only by engaging in the maltreatment. More study of the reasons for this abusive behavior is badly needed.
Q: What distinguishes MBP as a mental health issue of the perpetrator versus a criminal act of child abuse?
In 2013, the American Psychiatric Association opted to associate MBP with a mental disorder called “factitious disorder imposed on another” (FDIA). People with FDIA fabricate or induce illness in another person (or pet) by deceiving health care professionals and others. Increasingly, however, the term “medical child abuse” (MCA) is being used to make it clear that the behavior is abusive; and, in my opinion; not every perpetrator who engages in MCA has FDIA. For instance, some are delusional, and actually believe the child is sick without meaning to deceive others. Still, the behavior constitutes abuse, and would still qualify as MCA. Note that even falsely reporting (i.e., making up) an illness can be very serious if doctors perform procedures and prescribe medications as a result. Also, perpetrators who “simply” lie often progress to actually inducing illness if they don’t garner enough emotional gratification.
Q: What causes people to become MBP perpetrators?
There is no evidence that MBP is genetic or inborn. But many perpetrators claim to have experienced abuse or emotional neglect in childhood. If these claims are valid, some of them may have come to realize that the way to get attention and relief was to pretend to be sick. As adults, at least theoretically, they continue this same behavior but use the body of their child to get their needs met. Perpetrators almost universally have developed personality disorders, such as borderline personality disorder. That means that they have long-term, potentially self-defeating ways of coping with stressors. They may never have developed healthy mechanisms for doing so.